MaxillaryOvoid
Maxillary Second Premolar
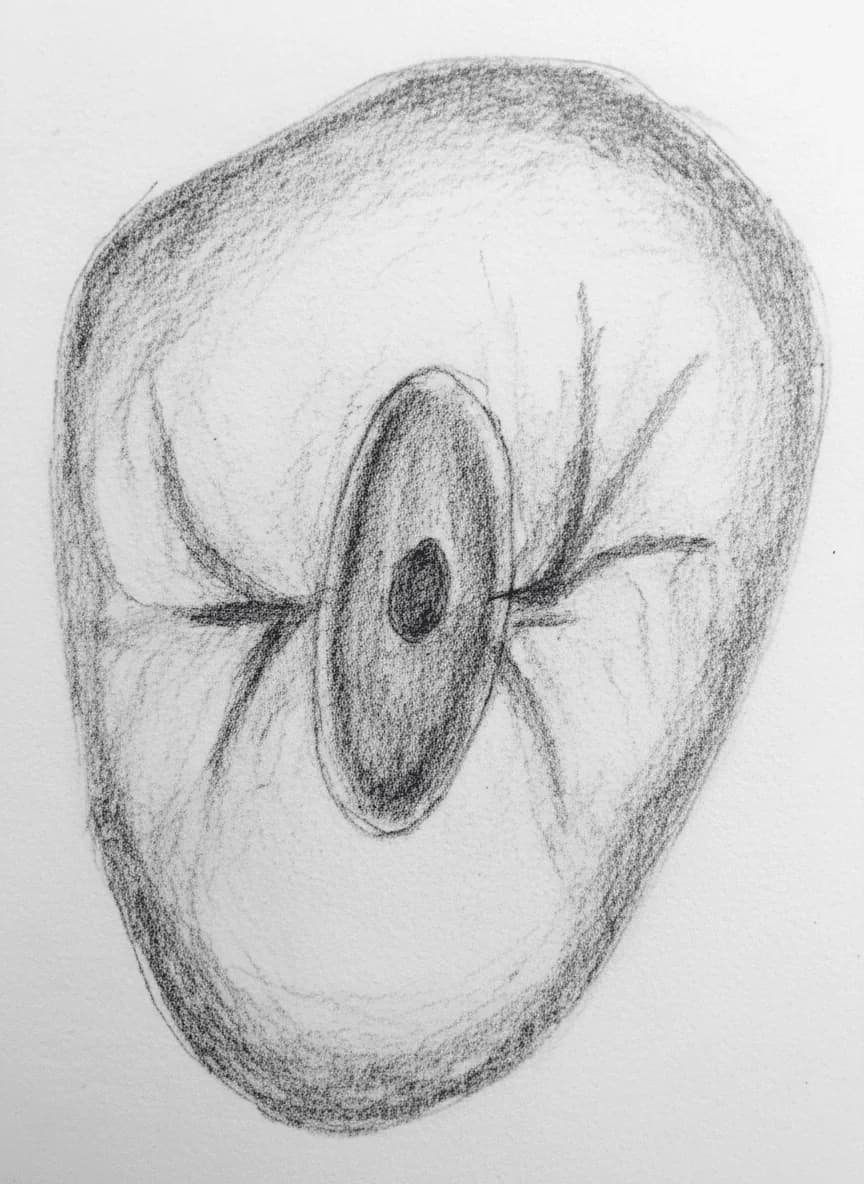
Maxillary Second Premolar - Axial View showing ovoid access cavity with variable canal anatomy (Vertucci Types I-IV)
Average Length21.5 mm
Root Development14 years
Universal #4, 13
FDI #15, 25
Access Cavity Design
ShapeOvoid
OrientationBuccopalatal; slightly wider mesiodistally than first premolar, reflecting more symmetrical crown
Entry PointCentral sulcus of occlusal surface
Landmarks
- Cusp tips define buccopalatal extension
- Central sulcus as longitudinal guide
Do Not Invade
- Mesial and distal marginal ridges (preserve structural integrity)
Canal Anatomy
Configurations
1 canal (Vertucci Type I)56-75%
2 canals joining apically (Vertucci Type II, 2-1)20-24%
2 separate canals (Vertucci Type IV, 2-2)10-20%
3 canals (Vertucci Type VIII)0.66-2%
Canal Positions
MCMain Canal
Often oval or ribbon-shaped (band-shaped), may appear as buccopalatal slot — always explore for second canal
BBuccal Canal
When 2 canals present; beneath buccal cusp tip
PPalatal Canal
When 2 canals present; beneath palatal cusp tip
Danger Zones
- ⚠Mesial concavity — similar to first premolar but generally less pronounced
- ⚠Strip perforation risk when 2-rooted, especially with aggressive buccal canal shaping
Clinical Tips
⚠️
Warning
Most anatomically variable maxillary premolar: Type I (56-75%), Type II (20-24%), Type IV (10-20%), Type VIII (0.66-2%)
⚠️
Warning
Slot-shaped orifice = assume 2 canals (Type II or IV) until proven otherwise — explore both walls
🔧
Technique
NaOCl bubble test at slot-shaped orifice helps confirm canal bifurcation
Anatomical Variations
Vertucci Type II (2-1 configuration)
20-24%Two canals originating from pulp chamber that merge into one canal before the apex with a single foramen. Isthmus region between canals harbors tissue.
Access Modification: Wider buccopalatal access to locate both orifices; NaOCl bubble test at isthmus; thorough irrigation of connecting area
Vertucci Type IV (2-2 configuration)
10-20%Two separate canals from pulp chamber to apex, each with its own foramen. May have separate roots or share a single root.
Access Modification: Extend access buccopalatally to achieve straight-line access to both canals
Three Canals (Type VIII)
0.66-2% (rare)Three separate canals (resembling molar configuration). Documented in case reports across multiple populations.
Access Modification: Extended access resembling molar preparation; CBCT recommended for mapping; microscope valuable